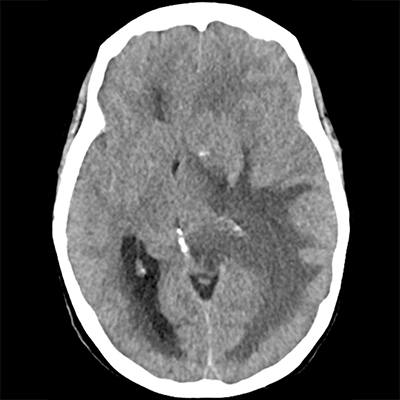
A 47 year-old woman presents with subacute functional decline. Beginning two months ago, she's developed a gradually worsening headache as well as progressive right-sided weakness. She and her family have noticed some additional word-finding difficulties. In the ED, she undergoes CT imaging. On this non-contrast head CT, you note a single possible underlying mass lesion with a significant amount of hypoattenuation within the temporoparietal lobe sparing the gray matter, as well as a larger occipital horn of the lateral ventricle and some periventricular hypoattenuation in that region as well. What is the most likely etiology of the periventricular hypoattenuation?
The time course given is discordant with this diagnosis, and the area is not a typical vascular territory for ischemia.
While periventricular hypoattenuation/leukoaraiosis is indeed a manifestation of chronic small-vessel ischemic disease, this would be of greater suspicion in an older patient with vascular risk factors. Patients with this degree of periventricular leukoaraiosis can also have ventriculomegaly, though it'd be ex vacuo (i.e. in the setting of diffuse cerebral volume loss)-- not the case here, as there's an obvious mass with marked perilesional edema causing ventricular entrapment as well as preserved cerebral volume.
It's possible to have leptomeningeal disease, even associated with primary CNS tumors such as GBM. However, the image suggests a clear asymmetric structural problem, with another diagnosis being more likely.
PRES is unlikely based on the clinical history given (subacute progressive symptoms, no risk factors). The white matter abnormalities associated with PRES can be confluent or non-confluent, and can also be asymmetric. However, the degree of mass effect demonstrated in this image would be highly unusual for PRES.
Yes! This patient has a newly-diagnosed brain tumor that has perilesional vasogenic edema out of proportion to its size. This mass effect has completely effaced the left-sided ventricular system and third ventricle, causing dilation of the right-sided ventricular system. The latter has become entrapped. This is effectively obstructive hydrocephalus. As a result of this increase in hydrostatic pressure, there is leakage of edema across the ependyma-- this is transependymal flow.
Copyright © 2024-2026 Andrew M. Nguyen, M.D. For educational use only.
This work is licensed under
CC BY-NC-SA 4.0.![]()
![]()
![]()
![]()