Great job! This patient's case was particularly challenging and required a mix of both type 1 and type 2 thinking. Our initial suspicion of seizures was reasonable, but later proved to be incorrect. In retrospect, after we were called back to see the patient due to continued clinical events, we could have asked ourselves whether or not the cEEG results were truly diagnostically satisfying. What question were we asking of the test, and how well could the test answer it? That could have been an opportunity to hit the brakes and ask ourselves: Are we missing some key information? Should we be considering another dangerous etiology?
It's not wrong to proceed with management of the most common cause if it's reasonably possible. However, we should be honest about the degree of uncertainty and whether there are any yellow or red flags. This can help us maintain vigilance as the case evolves, allowing us to be ready for key details to emerge that are subtle but could trigger a reevaluation and point us in the right direction.
We really had to challenge ourselves to avoid anchoring bias and to re-formulate the patient's presentation to come up with the correct diagnosis and management. Plateau waves are under-recognized, yet missing the diagnosis can be fatal.
When called to evaluate a patient for episodic neurologic signs/symptoms, it makes sense to think of common etiologies such as seizures and strokes. However, plateau waves are underappreciated and probably more common than we realize. Don't anchor and fall for the trap of evaluating only for seizure vs. stroke and then walking away. Consider whether something like intracranial hypertension could be the etiology, and whether anything in the patient's presentation could suggest a more ultimate cause for it.
The table below, from Chapter 3 of Plum and Posner's Diagnosis and Treatment of Stupor and Coma, lists the paroxysmal symptoms that have been reported to occur with plateau waves:
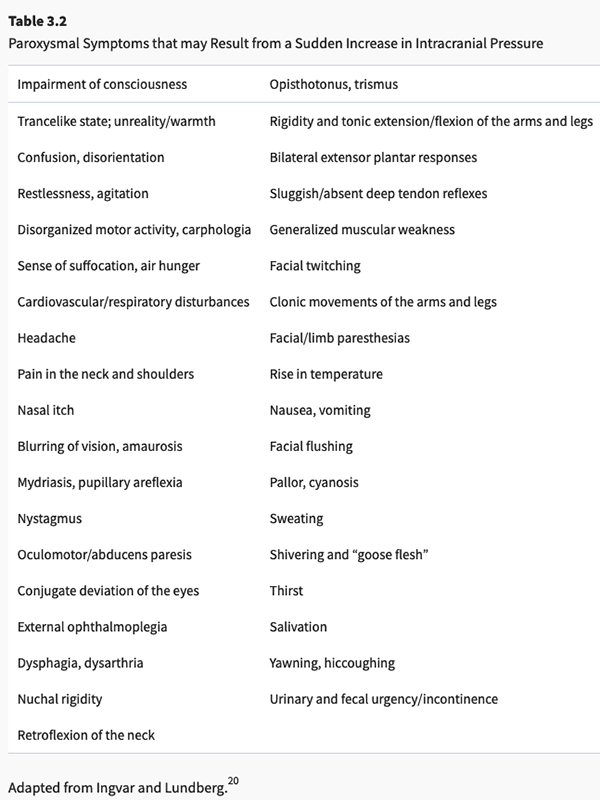
(Posner et al. 2019)
You'll notice how non-specific and, in some cases, non-focal, these symptoms are. Humbling. This also highlights how crucial it is to maintain a high index of suspicion for intracranial hypertension when invasive monitoring is not present.
Copyright © 2024-2026 Andrew M. Nguyen, M.D. For educational use only.
This work is licensed under
CC BY-NC-SA 4.0.![]()
![]()
![]()
![]()