The patient is stable enough to go to radiology to obtain an MRI of his brain.
 1/24
1/24
 2/24
2/24
 3/24
3/24
 4/24
4/24
 5/24
5/24
 6/24
6/24
 7/24
7/24
 8/24
8/24
 9/24
9/24
 10/24
10/24
 11/24
11/24
 12/24
12/24
 13/24
13/24
 14/24
14/24
 15/24
15/24
 16/24
16/24
 17/24
17/24
 18/24
18/24
 19/24
19/24
 20/24
20/24
 21/24
21/24
 22/24
22/24
 23/24
23/24
 24/24
24/24
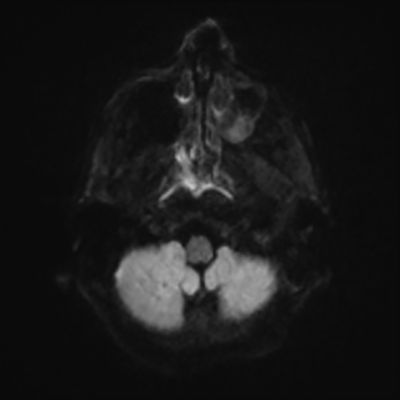
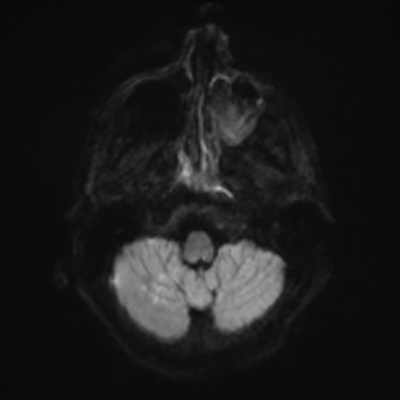
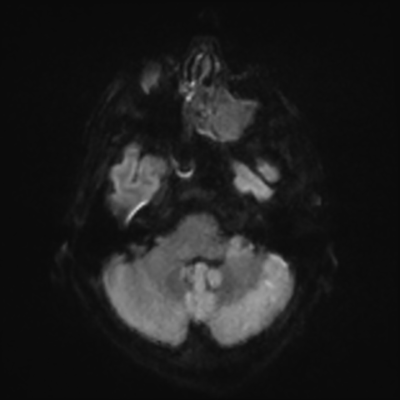
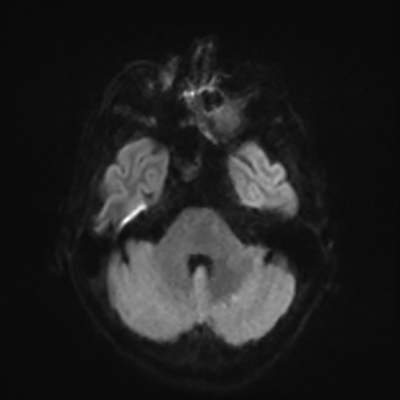
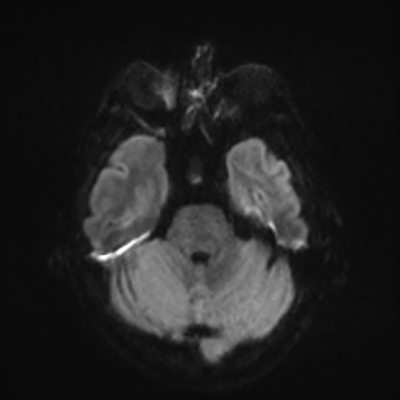
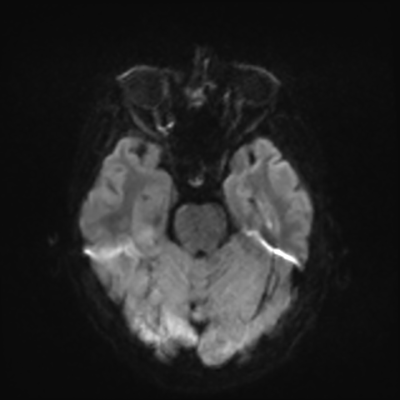
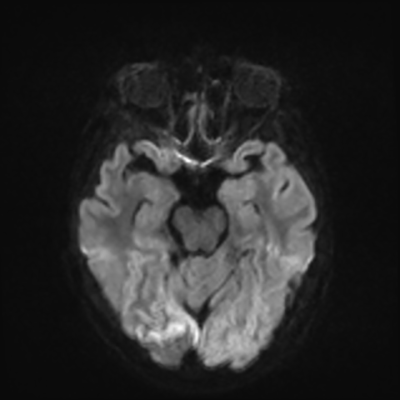
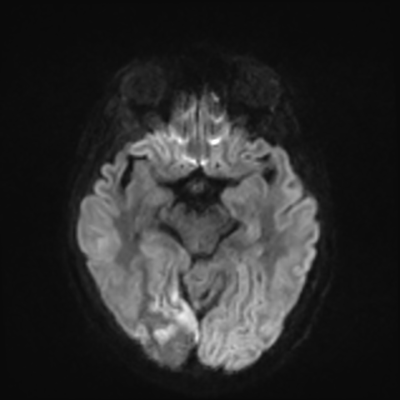
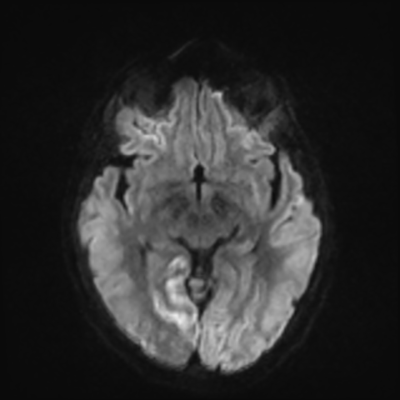
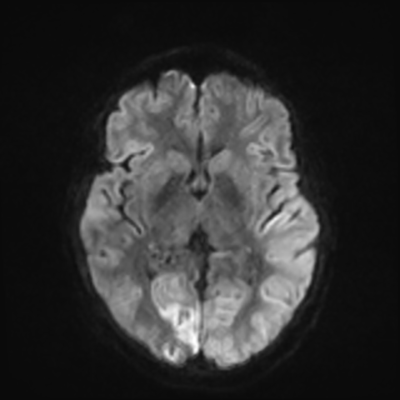
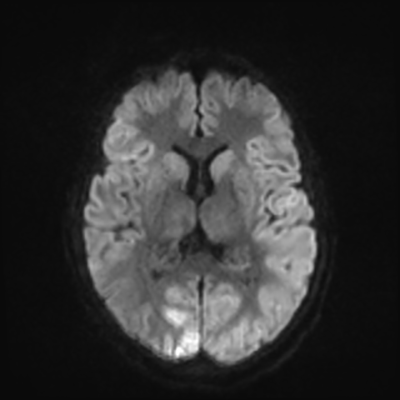
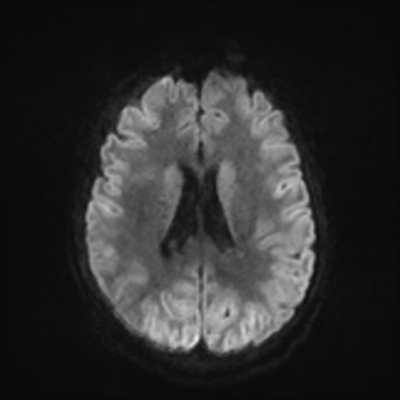
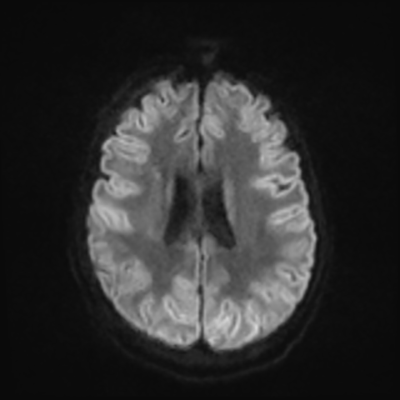
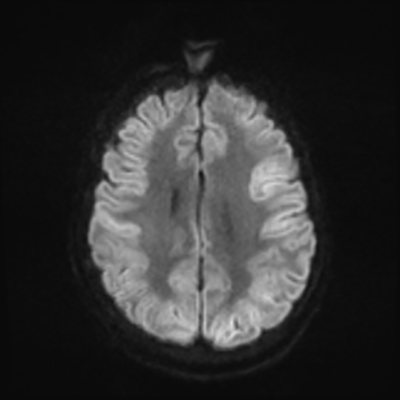
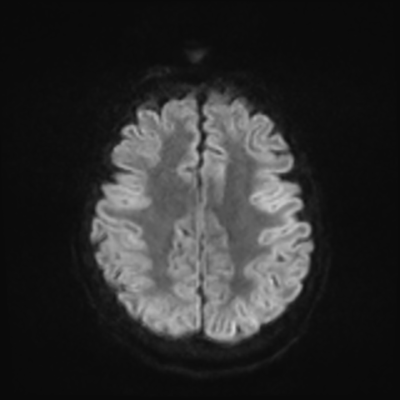
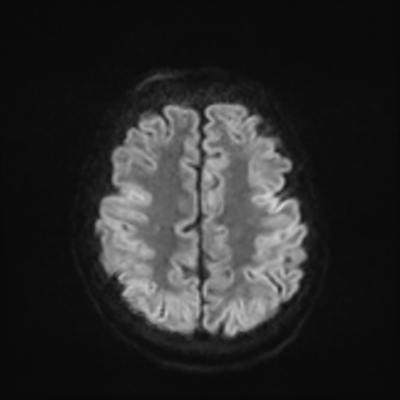
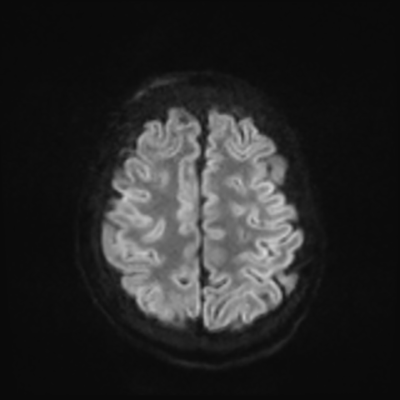
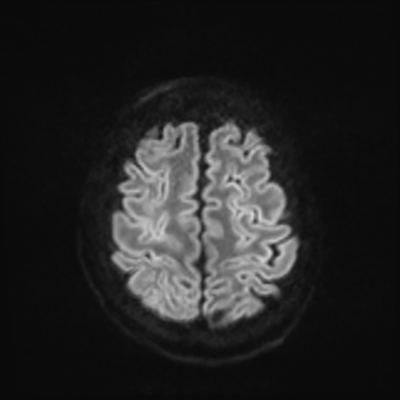
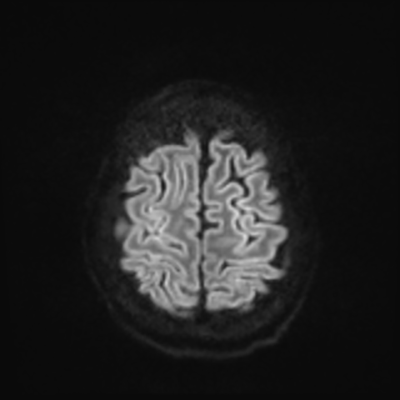
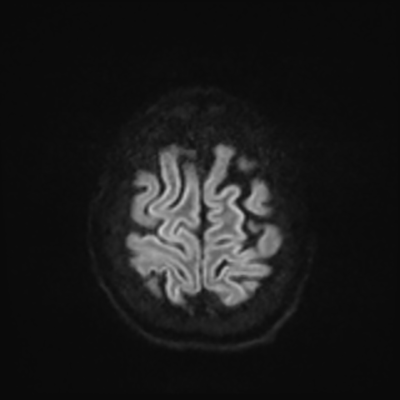
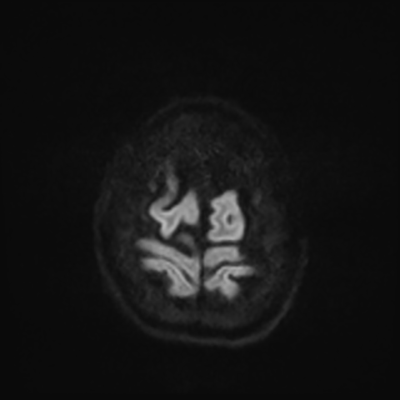
You can clearly see diffuse cortical and basal ganglia diffusion restriction, and that of his deep cerebellar nuclei as well. The right occipital lobe abnormalities are a little more prominent, but then you remember that he is known to have had a right occipital stroke weeks ago.
In reviewing his data, you know that he doesn't have any of the strong predictors of a poor neurologic prognosis. However, based on these findings on MRI, along with the absent reactivity on cEEG, you are able to tell the primary team and the patient's family that he is likely to have a poor prognosis, based on these multiple moderate predictors. Recovery is not completely impossible-- there is more uncertainty with this prognostication than if we were able to get SSEPs-- but you're very worried about his outlook and that any potential recovery would require a very protracted rehabilitation period. Given his high cervical cord injury level, tracheostomy would be required anyway. So, it comes down to whether his family thinks he'd want to pursue these aggressive measures.
Copyright © 2024-2026 Andrew M. Nguyen, M.D. For educational use only.
This work is licensed under
CC BY-NC-SA 4.0.![]()
![]()
![]()
![]()