DHC can reduce secondary injury by preventing continued compression of brain tissue. A meta-analysis of these trials confirmed that DHC improves 12-month mortality (70.2% vs. 28.8%, p < 0.00001, NNT 2.4). DHC also improves functional outcome at 12 months if the patient's age is < 60 and if they're treated within 48 hours of their stroke.
(Lin and Frontera 2021)
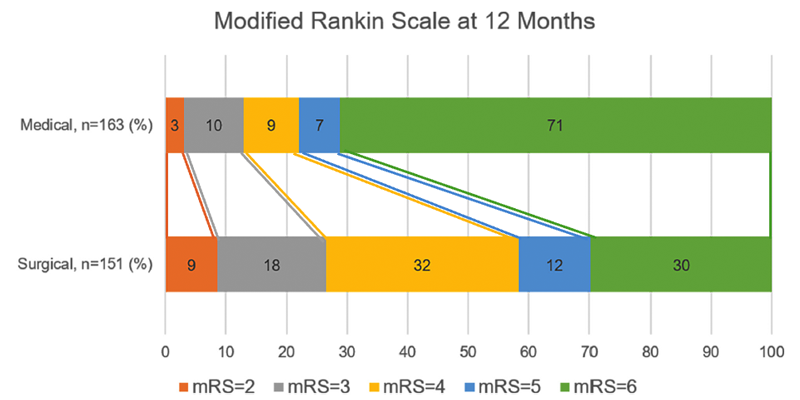
The above graphic shows the ordinal shift in mRS scores between the medical management arm and the surgical management arm. There are a few key interpretations of this graphic. For one, there's definitely more survivors across all functional outcomes (including good) as a result of DHC. However, a majority of patients-- though not all-- will still be dependent and unable to walk regardless of intervention. The most favorable outcome here is an mRS score of 2, not 0 or 1. It's sobering.
So, barring any surgical or patient-specific contraindications, DHC should generally be done early-- meaning within the first 48hrs-- for patients < 60, as there's both a morbidity and mortality benefit in this age group. While there could still be some functional benefit even if done after 48 hours, the optimal management would still be to perform this early. It's generally challenging to fully implement this data-driven approach because this strategy of being more proactive with surgery runs counter to the usual approach to neurosurgical interventions, with wanting to not operate unless patients absolutely need it. Being aware of this strong data is important for helping us ensure that patients get the right care. The AHA/ASA, NCS/AANS/CNS 2018 guidelines all recommend early DHC in accordance with this data.
Whether DHC should be done for patients aged > 60 is difficult. In this higher age group, DHC will still improve mortality, though at the cost of surviving with greater morbidity. This really needs to be emphasized when talking to families. Some patients might be okay with that trade-off. It's up to us to clearly explain this and elicit the patient's wishes as told through their family members.
Copyright © 2024-2026 Andrew M. Nguyen, M.D. For educational use only.
This work is licensed under
CC BY-NC-SA 4.0.![]()
![]()
![]()
![]()